
Many HealthTech startups and patient organizations check all the boxes for clinical rigor. They pull peer-reviewed papers, audit their local user testing, and build their product logic on a foundation of gold-standard clinical trials.
But there is a hidden trap in being "evidence-based" without critical review: inherited data bias.
If you rely on existing medical literature without critically appraising how that data was collected, you risk building your app’s algorithms, behavioral triggers, or symptom-tracking intervals on a monoculture. Many studies are built on highly resource-rich, homogenous patient cohorts. When you deploy that logic into the diverse, real-world healthcare landscape, you risk perpetuating health disparities, missing critical behavioral insights, and ultimately failing to serve the very patients your product is intended to help.
To clear the mHealthBelgium Level M3 hurdle and secure permanent INAMI/RIZIV reimbursement, you need a strategy that moves beyond standard regulatory checklists. It requires a three-part behavioral science framework:
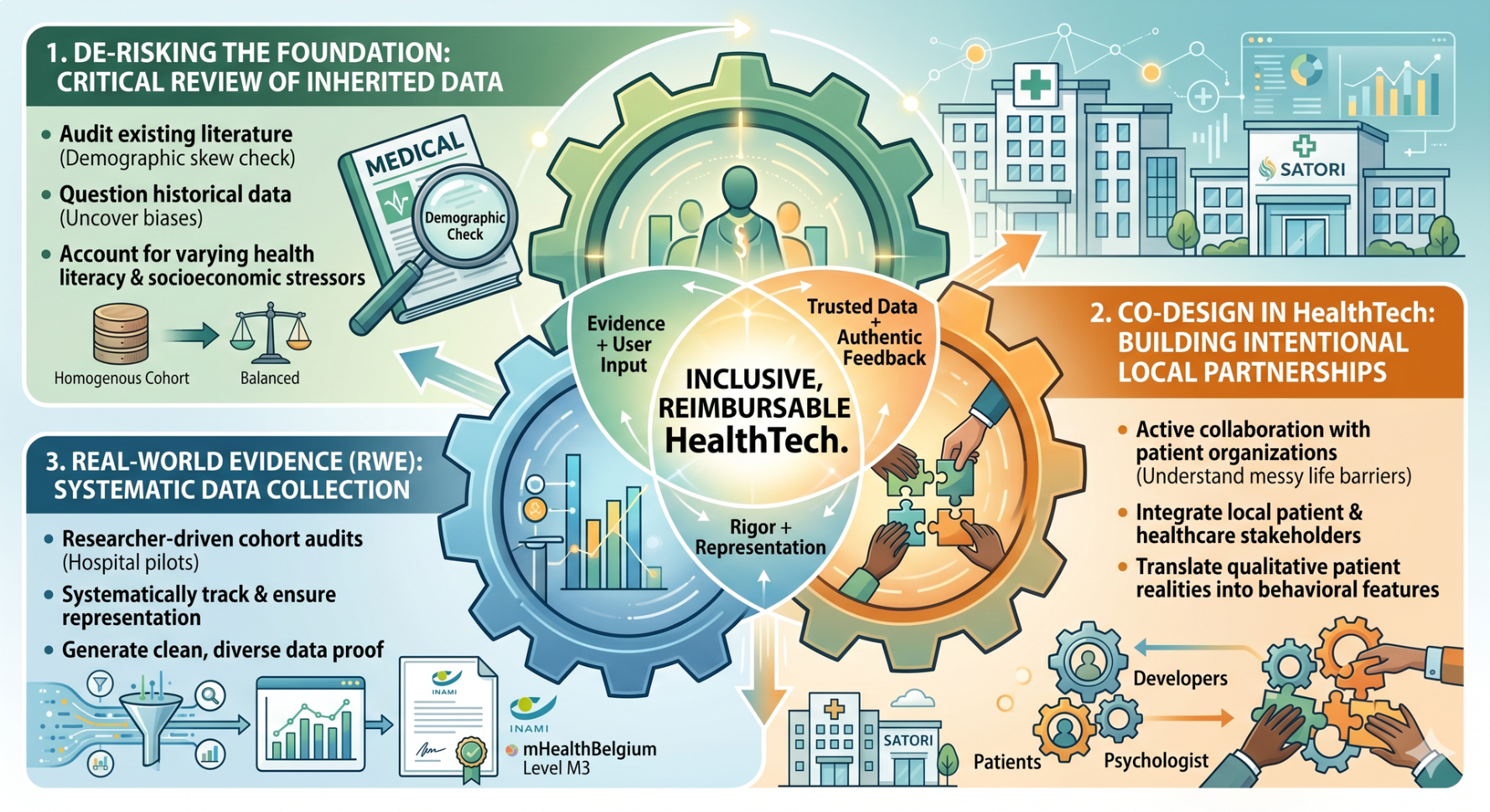
1. De-Risking the Foundation: Critical Review of Inherited Data
Don't treat peer-reviewed literature as universal truth. If your foundational data is built on a narrow snapshot of the population, your product introduces massive technical and clinical risk before you even write your first line of code or develop your first prototype. You must take a critical look beneath the surface to ensure your foundation accounts for real-world barriers like varying health literacy and socioeconomic stressors.
For researchers!
Check out this (very wonderful) paper by Alex Tremblay-McGaw on how to increase transparency regarding your sample demographics
2. Co-Design in HealthTech: Building Intentional Local Partnerships
You cannot design an effective digital care pathway in a vacuum. To understand the actual, messy life barriers patients face—such as shift-work schedules or historic mistrust of medical authority—you must actively prioritize co-design in HealthTech by partnering with local patient organizations and healthcare stakeholders. A health psychologist can help you translate these qualitative patient realities into concrete behavioral features.
For stakeholders!
Read more about the why and how of getting involved in co-design
[insert link to Satori blog]
3. Real-World Evidence (RWE): Systematic Data Collection for M3 Validation
To prove socio-economic added value to validation committees, you cannot rely on a highly skewed pilot study. By utilizing a researcher-driven cohort audit early in your hospital pilots, you systematically track and ensure representation. This generates the clean, diverse Real-World Evidence (RWE) required for health technology assessment in Belgium and permanent market access.
The Takeaway: Market access isn’t just about regulatory compliance; it’s about mastering behavioral science. By auditing the literature you inherit, co-designing with local networks, and systematically measuring cohort data, you build a viable, reimbursable business.
Want to audit your foundational research before your next pilot? Let’s connect for a consultation.